Access to Dental Care in Medicaid: Spotlight on Nonelderly Adults
Introduction
Oral health is a vicious though mostly ignored member of altogether health and well-being. Although good verbal health can be achieved by surety care, unchanging self-care, and a early detection, treatment, and government of problems, many people humour from bad verbal health, that mostly has additional inauspicious effects on their ubiquitous health and peculiarity of life. The superiority of dental illness and tooth detriment is disproportionately high among people with low income, reflecting miss of entrance to dental coverage and care. Racial and racial disparities in these measures are also pronounced.
Medicaid, a vital health coverage module for low-income Americans, provides a singly endless imperative advantage package for children that includes verbal health screening, diagnosis, and diagnosis services. In a final decade, with sovereign and state leadership, Medicaid and a Children’s Health Insurance Program (CHIP) have finished critical swell in addressing gaps in low-income children’s entrance to dental care, boosting children’s use of surety and primary dental services. However, even with a strong advantage package, securing entrance to dental providers and services has remained a pivotal challenge. The conditions for low-income adults in Medicaid is some-more formidable than that for children. Dental advantages for Medicaid adults are not compulsory by sovereign law, though are offering during state option, and many states yield usually singular coverage – in many cases, singular to extractions or puncture services. Further, when states have faced check pressures, adult dental services in Medicaid have typically been among their initial cutbacks. It is noteworthy, too, that a Medicare program, that covers aged adults and nonelderly adults with disabilities, provides no dental benefits.
Comprehensive coverage of dental caring for children in Medicaid and CHIP, as good as a nomination of pediatric dental caring as one of a 10 essential health advantages (EHB) underneath a Affordable Care Act (ACA), prove approval among policymakers of a significance of verbal health. New opportunities now exist to settle likewise strong verbal health advantages for low-income adults. Broad state coherence to conclude Medicaid advantages for adults, a ACA enlargement of Medicaid to nonelderly adults adult to 138% of a sovereign misery spin (FPL), and Medicaid remuneration and smoothness complement remodel are pivotal process levers. To assistance surprise sovereign and state movement concerning adult entrance to verbal health care, this brief examines a verbal health standing of low-income adults, a dental advantages lonesome by state Medicaid programs, and low-income adults’ entrance to dental caring today.
Why adult verbal health is important
Untreated verbal illness can have critical inauspicious impacts. Untreated verbal health problems can impact ardour and a ability to eat, or lead to tooth loss, all of that can lead, in turn, to nourishment problems. Untreated problems can also means ongoing pain that can impact daily activities such as discuss or sleep. Research has also identified associations between ongoing verbal infections and diabetes, heart and lung disease, stroke, and bad birth outcomes. Oral health problems can also meddle with work; employed adults are estimated to remove some-more than 164 million hours of work any year due to verbal health problems or dental visits. Adults who work in lower-paying industries, such as patron service, remove dual to 4 times some-more work hours due to verbal health-related issues than adults who have veteran positions. Visibly shop-worn teeth or tooth detriment can also mistreat office prospects for adults seeking work.
Dental illness superiority in nonelderly adults
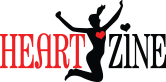
Nationally, 27% of all adults age 20-64 have untreated dental caries, though a weight of illness is not distributed uniformly in a population. The rate of untreated dental caries is top (44%) among adults with income subsequent 100% FPL ($11,880 per year for an sold in 2016) –more than twice a rate (17%) among adults with income during or above 200% FPL (Figure 1). Racial and racial minorities were also disproportionately influenced by verbal health problems. Both Black and Hispanic adults had significantly aloft rates of untreated caries than Whites, mostly a thoughtfulness of their aloft rates of poverty.
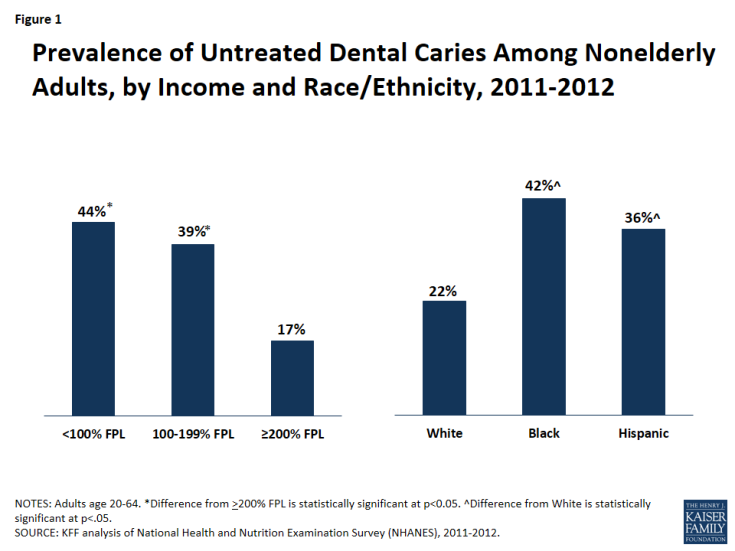
Figure 1: Prevalence of Untreated Dental Caries Among Nonelderly Adults, by Income and Race/Ethnicity, 2011-2012
Medicaid’s purpose in covering low-income adults
In 2014, Medicaid lonesome scarcely 28 million low-income nonelderly adults. The module covers 4 in any 10 nonelderly adults underneath a misery level. As of Feb 2016, 31 states and DC had adopted a Affordable Care Act’s (ACA) Medicaid expansion, that provides Medicaid eligibility to scarcely all adults with income during or subsequent 138% FPL ($16,394 per year for an sold in 2016); 19 states have not adopted a Medicaid expansion. The uninsured rate among low-income adults stays high, generally in non-expansion states. Across non-expansion states, a median Medicaid income eligibility for relatives is 44% FPL, and adults though contingent children, solely profound women and people with disabilities, are released from Medicaid no matter how bad they are. An estimated 2.9 million adults with income subsequent 100% FPL tumble into a “coverage gap” opposite non-expansion states – though entrance to Medicaid coverage and incompetent to validate for subsidies in a Marketplace.
Medicaid dental advantages for adults
States have substantial choice in defining Medicaid adult dental advantages given these services are optional, not mandatory, underneath sovereign Medicaid law. Adult dental advantages are a state choice opposite a house – for adults who validate for Medicaid underneath pre-ACA law and also for adults newly authorised for Medicaid underneath a ACA expansion. States contingency yield Alternative Benefit Plans (ABPs) for Medicaid enlargement adults, modeled on one of 4 “benchmark” options specified in a law, including an choice for coverage certified by a HHS Secretary. All ABPs contingency embody a 10 essential health advantages (EHBs) determined by a ACA. Notably, a EHBs embody pediatric dental benefits, though not adult dental benefits. Many states have used a Secretary-approved coverage choice to heed a advantages they yield for enlargement adults with their advantages for adults in normal Medicaid, modifying them as required to approve with a EHB requirements. Of a 31 states and DC that have adopted a Medicaid expansion, all though dual states yield a same dental advantages for enlargement adults that they do for a normal adult Medicaid population. The dual exceptions are Montana and North Dakota. Montana provides singular dental advantages for a normal Medicaid adult population, though nothing for Medicaid enlargement adults; North Dakota provides endless dental advantages for normal Medicaid adults, though nothing for enlargement adults.
Almost all states (46) and DC now yield some dental advantages for adults in Medicaid (Figure 2 and Appendix). However, usually as blurb dental skeleton typically do, many state Medicaid programs set a limit on their per-person spending for adult dental advantages or levy caps on a series of certain services they will cover. The operation of Medicaid adult dental advantages varies widely by state. As of Feb 2016, 15 states supposing endless adult dental benefits, tangible as a endless brew of services including some-more than 100 diagnostic, preventive, and teenager and vital physic procedures, with a per-person annual output top of during slightest $1,000. Nineteen states supposing singular dental benefits, tangible as fewer than 100 such procedures, with a per-person annual output top of $1,000 or less. The remaining 13 states with any adult dental advantages lonesome usually dental caring for pain use or puncture caring for injuries, trauma, or extractions. Four states supposing no dental advantages during all. Even in states that yield some dental benefits, adult Medicaid beneficiaries might face high out-of-pocket costs for dental care, creation it formidable or unfit to afford.
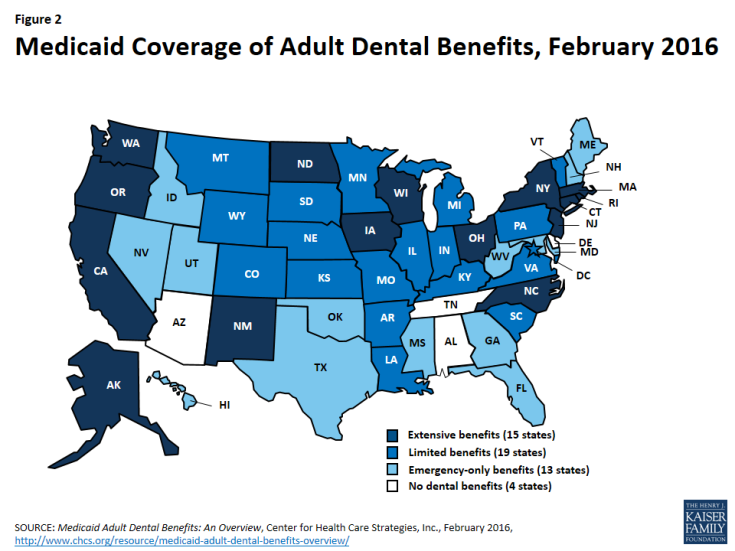
Figure 2: Medicaid Coverage of Adult Dental Benefits, Feb 2016
As discretionary Medicaid services, adult dental advantages are also theme to being cut. Many states change their advantages from one year to a next. In particular, when states are underneath check pressures, adult dental advantages in Medicaid have been cut behind and, when their economies improve, states mostly pierce to revive them. For example, in 2009, California separated coverage of non-emergency dental services for adults. In 2014, a state easy many of a benefits, including surety and physic care, periodontal services, and dentures. Similarly, Illinois separated coverage of non-emergency dental services for adults in 2012, though stretched services again in 2014 to embody singular fillings, base canals, dentures, and verbal medicine services. Research has shown that when states revoke or discharge adult dental benefits, unmet dental caring needs increase, surety dental use use decreases, and puncture dialect use for dental problems increases.
Adult entrance to dental care
Access to and use of dental caring among low-income adults depends on a series of variables. Medicaid eligibility for low-income adults, Medicaid coverage of dental benefits, the accessibility of dental providers, and customer and provider approval of a significance of surety dental caring all bear on either low-income adults obtain dental services. Particularly in a deficiency of dental benefits, cost is a categorical separator to entrance to dental caring for low-income adults. Paying for services out-of-pocket is difficult, if not impossible, on their stretched budgets. Over time, determined miss of entrance to dental caring or tie with dental providers might outcome in low expectations for verbal health among low-income adults, reinforcing existent disparities. And if consumers are unknowingly of a need for unchanging checkups or can't means them, they might wait until they knowledge verbal pain to find care.
Dental Care Utilization and Unmet Need
Regular dental caring is critical to progressing good verbal health. Low-income adults are reduction expected to have seen a dental provider within a final year than higher-income adults. In 2013, usually about 1 in 5 adults with income subsequent 200% FPL had a dental revisit in a past year, compared to 1 in 3 of those with income of 200-399% FPL, and 1 in 2 adults with income above 400% FPL (Figure 3). Similarly, adults with private dental coverage were some-more than twice as expected as adults with Medicaid/CHIP or uninsured adults to have seen a dental provider within a final year. (Note: “Uninsured” includes adults though private dental advantages or Medicaid and nonelderly Medicare-only adults who do not have private supplemental dental benefits.) In 2013, 49% of adults with private coverage had a dental revisit in a final year, compared to 20% of adults with Medicaid/CHIP and 17% of uninsured adults. Children in Medicaid/CHIP, for whom dental advantages are mandatory, were many some-more expected than adults in Medicaid to have had a dental revisit (42%). The low revisit rate for adults with Medicaid/CHIP coverage, compared to both children with Medicaid/CHIP and adults with private insurance, reflects, in part, a singular adult dental advantages lonesome in many state Medicaid programs.

Figure 3: Percentage of Nonelderly Adults with a Dental Visit in a Past Year, by Income and Insurance Status, 2013
In new research, dental caring emerged as a use for that insured adults were many expected to news unmet need due to cost. This was generally loyal for low-income insured adults (Figure 4). Nearly one-third (31%) of full-year-insured nonelderly adults with income during or subsequent 138% FPL and one-quarter (24%) of those between 139% and 399% FPL reported an unmet need for dental caring due to cost, compared to 11% of full-year-insured adults with income during or above 400% FPL. Also, nonelderly adults with open insurance, including those with Medicaid/other state coverage and those with Medicare, were some-more than twice as expected to news an unmet need for dental caring due to cost as adults with employer-sponsored word (35% vs. 16%) – again, expected reflecting singular Medicaid adult dental advantages in many states.
Figure 4: Unmet Need for Dental Care Due to Cost in Past 12 Months Among Full-Year Insured Nonelderly Adults, Mar 2015
Provider Availability and a Role of Health Centers
As of Jan 1, 2016, there were scarcely 49 million people vital in over 5,000 dental health veteran necessity areas (HPSAs) opposite a country. HPSAs are tangible radically in terms of a series of dental health professionals relations to a population. Although there is some discuss about either a inhabitant necessity of dentists exists, many experts determine that there is a geographic maldistribution of dentists and a necessity of office-based dentists accessible to yield low-income and special needs populations, including people in nursing homes and other residential institutions. In addition, dentist appearance in Medicaid is limited, as a vast commission of dentists accept no word and many dentists who do accept private word do not accept Medicaid. Medicaid beneficiaries mostly have problem anticipating a dental provider. The reasons dentists generally bring for not participating in Medicaid are low remuneration rates, executive burden, and high no-show rates among Medicaid patients.
Medicaid dental services might be delivered and paid for on a fee-for-service basement or by endless or dental-only managed caring skeleton that agreement with a state. Of a 39 states with endless Medicaid managed caring in 2015, 29 states reported that they cover adult dental benefits. Of these states, 10 states reported carving-out adult dental advantages to Medicaid fee-for-service or prepaid health plans.
Although many dental caring is supposing in solo or tiny office-based dental practices, village health centers are an critical source of dental caring for Medicaid beneficiaries and others in low-income, medically underserved communities. In 2014, health centers opposite a nation served 22.5 million patients, a vast infancy of them Medicaid beneficiaries (46%) and uninsured patients (28%). The ACA finished a vital investment in health core growth, establishing a five-year $11 billion Health Center Trust Fund (which has given been extended by 2017), and providing $1.5 billion in new appropriation for a National Health Service Corps, that reserve many of a medical and dental providers who staff health centers. Health centers can also agreement with private dental practices to yield verbal health services to health core patients. Between a ACA trust account dollars and augmenting studious revenues generated by stretched coverage for low-income people underneath a ACA, health centers in all states have been means to raise their use capacity; a new consult of health centers found that those in Medicaid enlargement states were significantly some-more expected than those in non-expansion states to have stretched their dental and mental services ability given a start of 2014. In 2014, over three-quarters of health centers supposing dental care, and about 15% of all health core studious visits were for dental services.
One devise with intensity to boost entrance to dental caring in low-income communities is to rise a some-more opposite verbal health workforce, given minority providers are some-more expected to work in minority communities and to yield caring to a underserved. Programs like a National Dental Pipeline Program have augmenting enrollment of under-represented minority students during participating dental schools. In addition, dental propagandize accreditation standards have been revised to urge farrago among dental propagandize expertise and students.
Expanding a Supply of Dental Care: Scope-of-Practice New Provider Types
In serve to dentists, dental hygienists, who specialize in surety caring and verbal hygiene, are an constituent partial of a dental workforce. Dental hygienists work in a accumulation of settings (e.g., private offices, schools, nursing homes) in suitability with varying state mandate for dentist supervision, formed on any state’s use acts or regulations. To raise entrance to dental care, some states have nice their scope-of-practice manners to concede dental hygienists to allow services though a participation or proceed organisation of a dentist. Accompanying changes might be indispensable in some states’ Medicaid remuneration policies and systems to assent dental hygienists to check a module directly for services supposing to Medicaid beneficiaries.
Some states have broadened a dental workforce serve by introducing new midlevel dental provider types. Conceptually, midlevel dental providers play a purpose identical to that of helper practitioners and medicine assistants in a medical caring context. They are partial of a dental veteran group and perform slight surety and physic services in a accumulation of settings. Three states – Alaska, Minnesota, and Maine – have famous and protected a new form of midlevel provider famous as a dental therapist, to assistance urge entrance to care, generally for underserved populations. Education requirements, roles, and organisation mandate for midlevel dental providers change opposite states. For example, Minnesota requires that during slightest 50% of a caseload of dental therapists and modernized dental therapists be Medicaid beneficiaries or underserved populations. Emerging investigate on midlevel dental providers indicates that they yield high-quality, cost-effective care.
Other strategies for optimizing stream dental caring ability are also developing. Effective Jan 1, 2015, California began requiring a Medicaid module to repay for services delivered by dental hygienists in conference with remote dentists, a use famous as “teledentistry.” This law was upheld years after a state began a Virtual Dental Home Demonstration Project, a commander module designed to exam a “virtual dental home” indication to raise entrance to caring in dental necessity areas. In this model, telehealth record is used to couple associated dental professionals operative in a village – purebred dental hygienists in choice practice, purebred dental hygienists, and purebred dental assistants – with dentists located in dental offices or clinics. The community-based providers collect studious information, including medical histories and cat-scan images, and this information is afterwards sent to a collaborating dentist. A diagnosis devise is developed, and a community-based provider furnishes a services they are certified to yield in a community, and patients requiring some-more formidable services are referred to a internal dentist.
Dental Delivery System
Important changes in dual pivotal realms are staid to impact a smoothness of dental caring in a entrance years. The initial relates to a classification of use delivery. Movement toward some-more integrated, “whole-person” caring and some-more accountable systems of caring (e.g., Accountable Care Organizations) is heading to arrangements in that providers who have not traditionally finished so are now pity studious information and collaborating in caring planning. Currently, states and smoothness systems (e.g., managed caring plans) are focused radically on integrating behavioral health caring with ubiquitous medical care, though some systems are holding stairs to confederate dental caring as well. Interestingly, early investigate indicates that ACOs that yield dental services are some-more expected to embody a health core and are many some-more expected to have contracts with Medicaid.
The second area of change is clinical caring itself. A opposite indication for verbal health caring is rising that departs from a normal fee-for-service, procedure-driven indication that prevails today, and instead involves caring formulation formed on sold studious characteristics and risk factors, and remuneration tied to peculiarity and outcomes, not volume. This proceed is radically a indication of impediment and ongoing caring management, in that studious risk is assessed, and surety care, early intervention, tighten monitoring, and caring government are targeted to people with or during high risk for disease. The aim is to urge verbal health outcomes by providing services formed on sold studious risk and need. Rethinking systems of caring and extended health complement burden might urge entrance to and function of dental caring as good as a impact of Medicaid spending for dental services.
Looking ahead
Improving a verbal health of low-income adults involves efforts to raise coverage, strengthen benefits, foster verbal health, and urge entrance and caring delivery. State Medicaid programs can play a vital purpose in this area and have critical levers for creation advances. States that have not nonetheless stretched Medicaid underneath a ACA have an event to cover millions of bad adults who miss other affordable health coverage options. Independent of a Medicaid expansion, improving state economies might raise a prospects for enlargement of adult dental advantages in Medicaid programs. The swell that states have finished in augmenting children’s entrance to and use of dental care, by building stronger provider networks, leveraging burden by contracts, and investing in caring coordination efforts, provides a substructure for identical movement for adults in Medicaid. States are also expanding a dental workforce by stealing scope-of-practice barriers and by targeted efforts among dental schools to boost farrago among dental students, as under-represented minority students are some-more expected to yield caring to a underserved. Finally, state Medicaid programs are implementing a horde of remuneration and smoothness reforms in office of higher-quality care, improved studious outcomes, and reduced costs. A executive importance of these new approaches is some-more integrated care, infrequently encompassing an stretched operation of health and amicable services and supports, as good as innovative workforce and other strategies for expanding access. With flourishing approval that verbal health is essential to altogether health and well-being, these new models of caring benefaction intensity for augmenting entrance to dental caring and improving dental caring and outcomes for both children and adults in Medicaid.
Appendix
Let’s retard ads! (Why?)

